About the Author
Dr. M. Zaman Khan graduated from Allama Iqbal Medical College (AIMC), Lahore, in the year 2008 and is an FCPS trainee in Medicine at JHL. Dr. Zaman took 2nd position in F.Sc. exams from Gujranwala board. He has topped University of Health Sciences, Lahore in third and final Professional Exams. He secured 14 gold medals in MBBS and was declared the ‘Most Distinguished Graduate 2002-07’. In 2008, he was declared ‘Star Laureate’ at national level by South Asia Publications.
 As a student, he deeply values innovation, research and high levels of professionalism. He was the recent successful participant of 60th Meeting of Nobel Laureate scientists held in Lindau, Germany, 2010, for which 692 young scientists were selected out of 40,000 applicants worldwide. He was also called to participate in prestigious Euro-Science Open Forum, Italy, 2010, in which only 50 out of 692 Lindau Fellows were selected. He would soon publish a book-size report on these events, narrating his intellectual participation and personal reflections, as a young Muslim scientist.
As a student, he deeply values innovation, research and high levels of professionalism. He was the recent successful participant of 60th Meeting of Nobel Laureate scientists held in Lindau, Germany, 2010, for which 692 young scientists were selected out of 40,000 applicants worldwide. He was also called to participate in prestigious Euro-Science Open Forum, Italy, 2010, in which only 50 out of 692 Lindau Fellows were selected. He would soon publish a book-size report on these events, narrating his intellectual participation and personal reflections, as a young Muslim scientist.
Apart from the academic and professional work, Dr. Zaman enjoys prose writing, biographical writing and poetry, mainly in Urdu, and English as well. He is soon going to publish his first work in Urdu poetry. He also devotes much of his time to spiritual and intellectual activities outside the boundaries of medicine science. He is founder of Society for Excellence in Education & Knowledge (SEEK). He is also in the advisory council of a student organization, ESEF-Pakistan.
Introduction
Primary stimulus of this work came from my teaching experience with final year medical students. Final year subjects are very vast in nature. Reading each and every book is all impossible a task to do. The relative importance of each topic needs to be assessed, otherwise the student may end up wasting a lot of time on non-important subjects.
There are three kinds of topics in terms of importance and chance of coming into exams, and each should be read according to its importance: 1st Rank Topics > 2nd Rank Topics > 3rd Rank Topics.
Time is a real limiting-factor. The critical task is how to prepare maximum number of important topics in less time. We would like to draw efficiency equation:
Efficiency (Success in Exams) = Output (No. of units learned) ÷ Input (Time)
Rank Order List (ROL), which I sketched above, has two features which students have found very useful for success: It prioritizes topics; and then guides student how to allocate time on the topics (which are mentioned in the book).
In-depth research has been done to calculate and find-out exactly what topics always come, ninety-percent of the times; and which come only ten-percent of the time. The percentage goes like this for ROL:
- 1st Order: 90% of exam comes from this section. It comprises of 40-45% of total syllabus.
- 2nd & 3rd: Only 10% of questions belong to this group. It covers 55% of the syllabus!
Nonetheless, ROL also solves a major problem that pupils face while studying: Problem of multiple book-reading. The argument goes like this: How can one study so many books when it is so difficult to read only one? 1st rank topics require reading multiple books the most. So for example, it is advisable to read Davidson for all topics of Medicine and to consult CMDT or Harrison for 1st order questions.
Out of 2nd order topics many MCQs and a few SEQs are picked. You need very less to study multiple books; but still these topics are important.
3rd order topics don’t require multiple reading, principally. A few MCQs are selected from this category.
Many students have found this guidebook very useful and have given me their feedback about how much ease ROL brought to their lives. I hope it would give you right direction and help you make better professionals.
Final Note
In the end, a word of caution: Medicine is still beyond this list of topics that are mentioned in this booklet.
Acknowledgement
It would like to pay special thanks to my junior colleagues Ayaz & Tayyab who helped me organize this rank order list. I would also like to thank all those who supported and encouraged me. I want to thank my parents who always encouraged me and prayed for me days and nights.
Table of Contents
Medicine
Surgery
Obstetrics & Gynaecology
Pediatrics
Medicine
RANK ORDER OF TOPICS OF MEDICINE IN ORDER OF IMPORTANCE FOR SEND UP AND ANNUAL EXAMINATION
Number of Questions from Each Unit
This table shows number of questions that are asked in the written examination.
NAME OF UNIT NUMBER OF QUESTIONS
- GIT 2
- LIVER 1
- CVS 2
- INFECTIOUS DISEASES 2
- ENDOCRINOLOGY AND DIABETES 2
- RENAL AND ACID BASE BALANCE 2
- PSYCHIATRY _ 2
- HEMATOLOGY 1
- CNS 1
10. RESPIRATION 1
11. RHEUMATOLOGY 1
12. DERMATOLOGY 1
GIT
1ST ORDER:
- Upper GIT bleed
- H. pylori & associated peptic ulcer disease
- Inflammatory bowel disease esp. Ulcerative colitis
- GERD
- CELIAC DISEASE
- Irritable bowel syndrome
2nd ORDER:
- Malabsorption syndromes. ( all)
3rd ORDER:
- Acute pancreatitis
LIVER
1ST ORDER:
- Hepatic encephalopathy
- Fulminant hepatic failure
- Ascites
- Portal hypertension
- HBV & HCV – Diagnosis and management
- Chronic liver disease
2nd ORDER:
- Investigating a jaundiced patient
- Hepato renal syndrome
- Wilson’s disease
3rd ORDER:
- Sclerosing cholangitis
- Primary billiary cirrhosis
- Autoimmune hepatitis
- Bud Chiarri syndrome
- Hemochromatosis
4th ORDER:
- Liver abscess
CVS
1st ORDER:
1. Acute MI
- Chest pain
- Acute dyspnoea
- Acute pulmonary edema
- CCF
- Atrial fibrillation
- Mitral regurgitation
- Hypertrophic cardiomyopathy
- Mitral stenosis
- Acute rheumatic fever
- Infective endocarditis
- Pericarditis & cardiac tamponade
- Pulmonary thromboembolism
2nd ORDER:
- Hypertension
- Sudden cardiac arrest
- Aortic dissection
3rd ORDER:
- Aortic regurgitation
- Aortic myxoma
INFECTIONS
1st ORDER:
- Pyrexia of unknown origin
- Enteric fever
- Malaria
- Tuberculosis
- Tetanus
- Meningitis
- Streptococcal infection
- Clostridial infections
- Acute diarrhea
- General aspects of HIV/AIDS
2nd ORDER:
- Chicken pox
- Infectious mononucleosis
- Dengue fever
- Diphtheria
- Hookworm infection
- Measles
- STD’s
3rd ORDER:
- Pneumocystis carnii
ENDOCRINOLOGY AND METABOLISM
1st ORDER:
- Addison’s disease
- Myxedema ( especially myxedema coma)
- Hyperthyroidism
- Acromegaly
- Cushing Syndrome
- Pheochromocytoma
- Sheehan’s syndrome / Panhypoparathyroidism
- Metabolic syndrome X
- Hyperlipidemias
2nd ORDER:
- Thyroiditis
- Diabetes Insipidus
- Thyrotoxicosis & Pregnancy
- Hypoglycemia
3rd ORDER:
- MEN syndrome
- Hyperparathyroidism
- Porphyrias
DIABETES
1st ORDER:
- Definition
- Diabetic ketoacidosis
- Complications of diabetes
- Diabetic neuropathy (especially autonomic neuropathy)
2nd ORDER:
- Non-ketotic hyperosmolar coma
RENAL
1st ORDER:
- Chronic renal failure
- Acute renal failure
- Renal replacement therapy
- Tubulo-nterstitial nephritis
2nd ORDER:
- Nephrotic syndrome (genral)
- Nephrotic syndrome
- Proteinuria
- Renal artery stenosis
- Post streptococcal glomerulonephritis
- IgA nephropathy & Henoch-Shonlein purpura
- Membranous glomerulonephritis
ACID BASE & ELECTROLYTES
1st ORDER:
- Hyponatremia
- Hypokalemia & hyperkalemia
- Hypeprcalcemia
- Interpretation of acid-base balance
2nd ORDER:
- Metabolic acidosis & alkalosis
PSYCHIATRY
1st ORDER:
- Schizophrenia
- Bipolar disorder
- Anxiety disorder (panic attacks)
- Conversion disorders
- Dementia
2nd ORDER:
- Somatization disorder
- Delirium
3rd ORDER:
- Personality disorders
HEMATOLOGY
1st ORDER:
- Investigating anemic patients
- Iron deficiency anemia
- Megaloblastic anemia
- Acute myeloblastic leukemia
- ITP
- Multiple myloma
- Aplastic anemia
2nd ORDER:
- Lymphoma
- Splenomegaly
- TTP
- Paroxysmal nocturnal hemoglobinuria
- Hereditary spherocytosis
- Thalassemia
- Hemophilia
- Von Willibrand disease
- DVT
CNS
1st ORDER:
- Meningitis
- Stroke
- Epilepsy (especially status epilepticus)
- Guillian-Barre syndrome
- Myasthenia gravis
- Parkinson’s disease
2nd ORDER:
- Multiple sclerosis
- Headache (especially migraine)
- Transverse myelitis
- Encephalitis
3rd ORDER:
- Space occupying lesion
- Cerebral venous thrombosis
- Motor neuron disease
- Trigeminal neuralgia
RESPIRATION
1st ORDER:
- COPD
- Acute asthma
- Community acquired pneumonia
- Bronchiactasis
- Pleural effusion
- Acute dyspnOea & hemoptysis
- Pulmonary thromboembolism
- Artificial respiration & assisted ventilation
2nd ORDER:
- Sarcoidosis
- Fibrosing alveolitis
3rd ORDER:
- Bronchogenic carcinoma
RHEUMATOLOGY
1st ORDER:
- Rheumatoid arthritis
- Osteoarthritis
- SLE
- Ankylosing spondylitis
- Gout
- Giant cell arthritis
- Reactive arthritis
2nd ORDER:
- Septic arthritis
- Other seronegative spondyloarthropathies
- Wegner’s & polyartritis nodosa
- Other vasculitis
3rd ORDER:
- Systemic sclerosis
- Polymyositis
- Polymyalgia Rheumatica
DERMATOLOGY
1st ORDER:
- Scabies
- Eczema
- Psoriasis
- Acne vulgaris
2nd ORDER:
- Skin bacterial infections
- Fungal infection
- Erythema nodosum
- Pyoderma gangreonosum
- Blistering diseases
3rd ORDER:
- Bullous pemphigoid
- Pemphigus vulgaris
Surgery
RANK ORDER OF TOPICS OF SURGERY IN ORDER OF IMPORTANCE FOR SEND UP AND ANNUAL EXAMINATION
Number of Questions from Each Unit
This table shows number of questions that are asked in the written examination.
NAME OF UNIT NUMBER OF QUESTIONS
1. GIT & ABDOMEN _ 4
2. UROLOGY 2
3. BREAST 1
4. THYROID & OTHER ENDOCRINE 1
5. THORACIC 1
6. CARDIAC 1
7. HEAD & NECK & OROPHARYNGEAL _ 1
8. NEUROSURGERY 1
9. ORTHOPEDICS 1
10. VASCULAR SURGERY 1
11. TRAUMATOLOGY 1
GIT & ABDOMEN
OESOPHAGUS
1ST ORDER:
- Esophageal carcinoma
- Corrosive injury
- Esophageal perforation
- Achalasia cardia
2nd ORDER:
- GERD (complication & treatment)
- Hiatus hernia
STOMACH & DUODENUM
1ST ORDER:
- Peptic ulcer & it’s complications especially perforation
- Gastric outlet obstruction & Hypertrophic pyloric stenosis
- Gastric carcinoma
LIVER
1st ORDER:
- Liver abcess (Pyogenic & Amaebic)
- Hydatid cyst
2nd ORDER:
- Hepatic trauma
3rd ORDER:
- Surgical treatment of portal hypertension
SPLEEN
1st ORDER:
- Splenic trauma
- Spleenectomy (Indications, Procedure, Prophylaxis & Complications)
2nd ORDER:
- Spleenomegaly
GALLBLADDER AND BILE DUCT
1st ORDER:
- Acute cholecystitis
- Gallstones & its complications
- Ascending cholangitis
- Choledocholithiasis
2nd ORDER:
- Causes of obstructive jaundice
- Bile duct injury
PANCREAS
1st ORDER:
- Acute pancreatitis
- Pseudopancreatic cyst
2nd ORDER:
- Carcinoma of head of pancreas
- Chronic pancreatitis
- Zollinger-ellison syndrome & Gastrinoma
SMALL AND LARGE INTESTINES
1st ORDER:
- Colorectal carcinoma
- Ulcerative colitis
- Intestinal tuberculosis
- Typhoid perforation
2nd ORDER:
- Meckel’s diverticulum
- Stomas
INTESTINAL OBSTRUCTION
1st ORDER:
- General complications and management
- Acute intussusception
- Volvulus
- Paralytic ileus
- Acute abdomen and its causes
VERMIFORM APPENDIX
1st ORDER:
- Acute appendicitis
- Appendicectomy
2nd ORDER:
- Carcinoid tumor
RECTUM
1st ORDER:
- Rectum carcinoma
- Rectal prolapse
ANAL CANAL
1st ORDER:
- Hemorrhoides
- Anal fissures
- Pilonidal sinus
- Fistula in ano
- Anorectal abscess
2nd ORDER:
- Imperforate anus
HERNIA AND ABDOMINAL WALL
1st ORDER:
- Burst abdomen and incisional hernia
- Progressive post operative bacterial synergistic gangrene
- Strangulated hernia
- Surgical anatomy of inguinal canal
2nd ORDER:
- Inguinal hernia
3rd ORDER:
- Epigastric hernia
- Umblical and paraumblical hernia
- Femoral hernia (rare)
PERITONEUM
1st ORDER:
- Acute peritonitis
2nd ORDER:
- Tuberculosis peritonitis
- Mesenteric cysts
- Tuberculosis of mesenteric lymph nodes
3rd ORDER:
- Pseudomyxoma peritonei
UROLOGY
1st ORDER:
- Hematuria
- Renal cell carcinoma
- Benign prostatic hyperplasia
- Urethral injuries
- Renal, ureteric and vesical stones
- Testicular tumors
- Acute urinary retention
- Renal trauma
- Hydronephrosis
- Testicular tortion
- Surgical anatomy of prostate
2nd ORDER:
- Wilm’s tumor
- Carcinoma of bladder
- Varicocele
- Hydrocele
- Fournier’s gangrene (scrotum)
3rd ORDER:
- Renal tubercuslosis
- Ureteric injuries
- Diverticulae of bladder
- Prostatic carcinoma
- Circumcision
THORAX
1st ORDER:
- Tension pneumothorax
- Chest trauma and chest intubation
- Thoracotomy
- Flail Chest
2nd ORDER:
- Empyema
- Hemothorax
CARDIAC SURGERY
1st ORDER:
- Cardiopulmonary bypass
- Cardiac temponade
- Aortic dissection
2nd ORDER:
- Valvular disease (From Ellis)
BREAST
1st ORDER:
- Breast carcinoma
(Staging, Management according to age & stage)
2nd ORDER:
- Fibroadenoma
3rd ORDER:
- Gynaecomastia
ENDOCRINE
1st ORDER:
- Multinodular goiter
- Carcinoma thyroid
- Solitary thyroid nodule
- Thyroidectomy (Indications,procedure,complications)
- Pheochromocytoma
2nd ORDER:
- Hyperparathyroidism
OROPHARYNGEAL
1st ORDER:
- Carcinoma tongue
- Pleomorphic adenoma
- Submandibular gland carcinoma
- Complication of salivary gland surgery
- Cleft lip & cleft palate
- Tuberculous lymphadenitis
- Mandibular trauma
2nd ORDER:
- Plunging ranula
- Sialadenitis
3rd ORDER:
- Types of neck dissection (from CSDT)
- Maxillary fractures
ORTHOPEDICS
1st ORDER:
- General orthopedics (complete)
- Fracture of
- Lower end of humerus
- Lower end of radius
- Neck of femur
- combined fracture of tibia & fibula
- Dislocation of hip joint
2nd ORDER:
- Osteosarcoma & briefly other tumors
- Chronic osteomyelitis
NEUROSURGERY
1st ORDER:
- Head injury
- Extradural hematoma
- Subdural hematoma
- Cervical spine injury
- Types of nerve injury
- Radial & ulnar nerve palsy
2nd ORDER:
- Subarachnoid haemorrhage
- Spine injuries
- Median nerve palsy
VASCULAR SURGERY
1st ORDER:
- Acute limb ischemia
- Gangrene
- Buerger’s disease
- Deep vein thrombosis
2nd ORDER:
- Varicose veins
- Lymphoedema
3rd ORDER:
- Amputation
TRAUMATOLOGY
1st ORDER:
- ATLS
- Blunt abdominal trauma
- Exploratory laparotomy
- Diagnostic peritoneal lavage
_____________________________________________________________
Note: For other topics of General surgery Consult
“General Surgery by Abdul Wahab Dogar ’’
GYNAECOLOGY & OBSTETRICS
OBSTETRICS
PHYSIOLOGICAL CHANGES IN PREGNANCY
1ST ORDER
- Systemic changes (volume homeostasis, blood, cvs)
- Endocrinological changes
2ND ORDER
- Remaining whole chapter (important)
ANTENATAL CARE
1ST ORDER
- Antenatal visits
- Antenatal history and examination
ANTENATAL IMAGING AND ASSESSMENT OF FETAL WELL BEING
1ST ORDER
1. Diagnostic ultrasound (esp. features during 3rd trimester)
- CTG
- Biophysical profile scoring
PRENATAL DIAGNOSIS
1ST ORDER
- Diagnosis of down’s syndrome
- Comparison of various pre-natal diagnostic procedures
2ND ORDER
- Neural tube defects
- Congenital heart defects
3RD ORDER
- Remaining chapter
ANTENATAL OBSTETRIC COMPLICATIONS
1ST ORDER
- Hyperemesis gravidarum
- APH Antepartum Hemorrhage (Placenta previa, Abruptio placentae)
- ECV
2ND ORDER
- Minor disorders of pregnancy
- UTI
- Venous thromboembolism
- Oligo and Polyhydroamnios
- Rh iso-immunization
3RD ORDER
- Abdominal pain in pregnancy
TWIN AND MULTIPLE GESTATIONS
1ST ORDER
- Definition
- Classification
- Complication
DISORDERS OF PLACENTATION
1ST ORDER
- Placenta previa
- Placental apruption
- PIH (Pregnancy Induced Hypertension) and Eclampsia
- IUGR (Intra-Uterine Growth Retardation)
PRETERM LABOUR
1ST ORDER
- Causes and Management
MEDICAL DISORDERS
1ST ORDER
- Anemia
- Thyroid dysfunction
- Hypertension
- Diabetes Mellitus
2ND ORDER
- Heart disease
3RD ORDER
- Epilepsy
- Perinatal infections (infection screening during pregnancy)
NORMAL LABOUR
1ST ORDER
1. Physiology of labour (dimensions)
- Definition of 3 stages of labour
- Management of all 3 stages of labour (esp. active management)
- Partogram
2ND ORDER
- Mechanism of labour
ABNORMAL LABOUR
1ST ORDER
- Breech presentation
- Obstructed labour and fetal distress
- The Bishop scoring
- Induction of labour
- Assisted delivery (forceps, ventouse)
2ND ORDER
- Pain relief in labour and different types of anaesthesia
- Episiotomy and C-Section
- Deep transverse arrest and transverse lie
3RD ORDER
- Perineal tears
- Shoulder dystocia
PUERPERIUM
1ST ORDER
- PPH
- Puerperial pyrexia
2ND ORDER
- Breast disorders
- Post partum psychosis
- APGAR score
 Obstetrics’ ‘Most Wanted’ Topics
Obstetrics’ ‘Most Wanted’ Topics
GYNAECOLOGY
1ST ORDER
- Amenorrhoea
- Menorrhagia (esp. fibroid uterus)
- Infertility
- Contraception
- Abortion (esp. septic abortion)
- Endometeriosis and adenomyosis
- CA cervix
- Ovarian CA
- Endometrial CA
- UV (Utero-Vaginal) prolapse
- Abnormal vaginal discharge
- Vaginal candidiasis
- Bacterial vaginosis
- Trichomoniasis
- Post menopausal syndrome and HRT
- Hysterectomy
- Dilatation & Curratage
- Laparoscopic surgery
2ND ORDER
- Urodynamic stress incontinence
- Detrouser over activity
- Normal menstrual cycle
- Benign tumors of ovary
- Bartholin cyst and other vaginal cysts
- Manchester repair
3RD ORDER
- Vulval CA
PEDIATRICS
IMMUNIZATION
1ST ORDER:
- EPI Schedule
- Details of all vaccines in EPI schedule
2ND ORDER:
- Meningococcal vaccine
- H.Influenza vaccine
- Pneumococcal vaccine
3RD ORDER:
1. Typhoid vaccine
2. Passive immunization
CNS
1ST ORDER:
- Meningitis
- Epilepsy
- Febrile fits
- Cerebral palsy
- Cerebral malaria
2nd ORDER:
- Encephalitis
- G.B syndrome
3rd ORDER:
- Hydrocephalus
- SOL esp. intracranial tumours and brain abscess
- Acute stroke
- Floppy infant
CVS
1ST ORDER:
- Tetrology of fallot
- Ventricular septal defect
- Patent ductus arteriosus
- Atrial septal defect
- CCF
- Infective endocarditis
2nd ORDER:
- Transposition of great vessels
3rd ORDER:
- Cardiomyopathy
RESPIRATORY SYSTEM
1ST ORDER:
- Acute respiratory infection severity classification
- Pneumonia
- Bronchial asthma
- Bronchiolitis
2ND ORDER
- Bronchiectasis
- Croup & Acute epiglottitis
3RD ORDER
- Pneumothorax
- Pleural effusion
GIT & LIVER
1st ORDER:
- Acute diarrhea
- Celiac disease
2ND ORDER
- Hepatomegaly
- Acute and chronic hepatitis
- IBD
HEMATOLOGY AND ONCOLOGY
1st ORDER:
- Thalassemia
- Aplastic anemia
- Hemophilia
- ALL and Hodgkin’s lymphoma
- Von Willibrand’s disease
- ITP
2nd ORDER:
- AML
- Non Hodgkin’s lymphoma
- Causes of Hepatomegaly and Splenomegaly
- Iron deffecieny anemia
- Megaloblastic anemia
3RD ORDER
- DIC
ENDOCRINE AND GENETICS
1st ORDER:
- Cretinism
- Down’s syndrome
- Diabetic ketoacidosis
- Rickets
2nd ORDER:
- Wilson’s disease
3RD ORDER
- Glycogen storage diseases
- Mucopolysaccharidosis ( esp. Hurler syndrome)
- Congenital adrenal hyperplasia
NEPHROLOGY
1st ORDER:
- Post streptococcul glomerulonephritis
- Nephritic syndrome and proteinuria
2nd ORDER:
- ARF
- CRF
3rd ORDER
- Electrolyte and acid base balance
- Hematuria
INFECTIOUS DISEASES
1ST ORDER:
- Rheumatic fever
- Acute diarrhea
- Enteric fever
- Measles
- Tuberculosis
- Diphtheria
- Tetanus
- Malaria
2ND ORDER:
- Poliomyelitis
- Chicken pox
- Pyrexia of Unknown Origin
3RD ORDER
- Worm infestation
- Mumps
NEONATOLOGY
1ST ORDER:
- Jaundice neonatorum
- Prematurity
- Neonatal sepsis
- Perinatal asphyxia
- Neonatal seizures
2ND ORDER:
- RDS
- Necrotizing enterocollitis
- Intra ventricular hemorrhage
- Hemorrhagic disease of newborn
3RD ORDER:
- Small for gestational age
- Hypocalcaemia
NUTRITION
1ST ORDER:
- Malnutrition ( kwashiorkor and marasmus)
- Breast feeding
MISCELLANEOUS
- IMCI (Integrated management of childhood illness)
Pediatrics’ ‘Most Wanted’ Topics
PART-2
CHECK LISTS OF CLINICAL METHODS IN MEDICINE
On Getting through the Short Cases
Performance in short cases is assessed at three levels.
- Efficient performance of the clinical methods.
- Proper description of the findings.
- Discussion (differential diagnosis, diagnosis, management) based on the theoretical knowledge.
It is important to note that most students try to master their theoretical knowledge, pay less attention towards efficient performance of clinical methods and least towards proper description of the findings. This is a drawback on their part. A deficiency in performing the clinical methods and poor description of findings hardly provide them a chance to show their ‘proficiency’ in theoretical knowledge.
This check list of clinical methods should be viewed as a humble effort to provide a guideline only. It neither includes examination of all the systems nor details of ‘how’ to perform the methods but a list of ‘what to do’. Students are encouraged to add to these lists or make their own lists of examination of other systems. Students should also orient them on ‘what to do when a specific command is given’.
I have also tried to ‘examplify’ the description of clinical findings whether it be in the long cases or the short cases. This ‘description’ in a proper way is ‘key’ to high performance, I have learnt over years. Another humble request to students is that they should write down the complete description of examination of a system for their long case. Just writing S1+S2+0 in the precordial examination leaves the worst impression on the examiner.
Be polite, humble but CONFIDENT.
Examination of Central Nervous System
Introduction & Consent
Greeting
Introduction and rapport
Consent (Explain what you are going to do)
Position
Exposure
Assess the Higher Mental Functions
Assess the orientation of the patient in time, place and person.
Assess the speech of the person.
Examination of the Cranial Nerves
Command no.1: Examine the Cranial Nerves of the Patient
You need to be concise. You are supposed to complete your examination in 3-4 min. Examine the patient in sitting position. Examiner should be at the level of the patient.
Check the gross visual acuity. (e.g. ask to read something written on the wall)
|
Assess the visual field (confrontation method)
|
Check the papillary light reflexes (Direct, Consensual, Swinging)
|
Perform Fundoscopic examination of eyes.
|
Check the extra-ocular muscle movements (by making an “H” after stabilizing the head)
|
Check the accommodation reflex.
|
Check the conjunctival reflex.
|
Check the gross sensation of the face (for three divisions of trigeminal nerve).
|
Check the power of the masseter muscles and ask patient to show his teeth.
|
Ask the patient to furrow his/her forehead.
|
Ask the patient to close his eyes against resistance.
|
Ask the patient to protrude his tongue. Ask him to move tongue to either side.
|
Ask the patient to open his mouth, check it with the torch and examine uvula. Ask the patient to say “aah” and check the movement of the palate and position of the uvula.
|
Ask the patient to shrug his shoulders against the resistance.
|
Command no.2: Examine the Optic Nerve of this Patient
|
Command no.3: Examine the Occulomotor Nerve
Check the pupillary light reflexes.
|
Check the accommodation reflex.
|
Check for ptosis. (Observe, Margin Reflex Distance MRD etc.)
|
Check the extra-ocular movements of the eyes.
|
Command no.4: Examine the Trigeminal Nerve
Check the corneal and conjunctival reflexes.
|
Check sensations of the face.
|
Check the power of the masseter.
|
Command no.5: Examine the Facial Nerve
Observe face of the patient for loss of nasolabial folds, mouth-deviation, dribbling of saliva, epiphora.
|
Ask the patient to furrow his forehead.
|
Ask patient to close his eyes: First without resistance. Then ask him to close eyes and not let you open them. Then ask him to open eyes and try to close them against resistance (to check for bell’s phenomenon.)
|
Check the Conjunctival reflex.
|
Ask the patient to show his teeth.
|
Ask the patient to puff-out his cheeks.
|
Examine the external auditory canal for any vesicular eruptions (Ramsay-Hunt Syndrome).
|
Ask patient to protrude his tongue, observe the tongue for vesicles, check the taste sensations of the anterior two-third of the tongue or tell the examiner that you would like to check it.
|
Command no.6: Examine the Motor System of Upper Limbs.
Expose properly.
|
Make position of the patient.
|
Observe both the arms calmly.
|
Ask for tenderness. Check for spontaneous muscle fasciculations under light. Then percuss muscle bulk to look for ‘elicited’ fasciculations.
|
Measure the muscle bulk.
|
Check tone of the muscles:
|
|
|
With supination and pronation.
|
|
Flextion and extension at elbow
|
|
Circumduction at shoulder joint
|
|
Check tone on the other side as well at the same time to compare the two.
|
Check the power of the muscles bilaterally:
|
Hands: At Thumb
|
|
|
Adduction of the thumb
|
|
Flexion of the thumb
|
|
Extension of the thumb
|
|
Opposition of the thumb
|
Hands: At Fingers
|
|
|
Check abduction of fingers
|
|
Check adduction of fingers (additional: check for formet’s sign)
|
Wrists
|
|
Elbow joint
|
|
|
Check extension
|
Shoulder joint
|
|
|
Check adduction
|
Check deep tendon reflexes bilaterally
|
|
|
Triceps reflex
|
|
Supinator jerk
|
|
Finger jerk
|
Perform finger nose test bilaterally.
|
Redrap the patient and say thanks.
|
Command no.7: Examine the Motor System of Lower Limbs
Expose properly.
|
Observe for posture and obvious wasting.
|
Check for muscle tenderness and fasciculations as in upper limb.
|
Measure the muscle bulk bilaterally.
|
Check tone of the muscles bilaterally.
|
|
|
At ankle joint
|
|
At knee joint
|
|
At hip joint
|
Check power of the muscles. (ask the patient to raise legs to assess the power grossly.)
|
At toes
|
Ankle
|
|
|
Plantar flexion
|
|
Inversion
|
|
Eversion
|
Knee
|
|
|
Extension
|
Hip
|
|
|
Extension
|
|
Abduction
|
|
Adduction
|
Check deep tendon reflexes
|
Ankle jerk
|
Knee jerk
|
Check for the clonus
|
Ankle clonus
|
Patellar clonus
|
Check for the plantar reflex (Babinski sign)
|
Perform heel-knee-shin test.
|
Ask patient to stand. Look for Pomberg’s sign.
|
Ask patient to stand from sitting position. (for proximal muscle weakness)
|
Ask patient to stand on his toes.
|
Ask patient to stand on his heel.
|
Ask patient to walk and note his gait.
|
Check for vertebral column pathology if weakness found.
|
Say thanks to the patient.
|
Command no.8: Examine Cerebellar System of the Patient.
Communicate with the patient and assess the speech.
|
Examine the eyes for nystagmus.
|
Look for arm drift and check tone of upper limb muscles.
|
Perform finger nose test to check for tremors and past–pointing.
|
Check for dysdiadochokinesia.
|
Check for the rebound phenomenon.
|
Examine tone of lower limbs.
|
Perform heel-knee-shin test.
|
Ask patient to fold arms and sit up to check for truncal atexia.
|
Test for the pendular knee jerk.
|
Test for the Romburg’s sign.
|
Ask the patient to walk and examine the gait.
|
Say thanks to the patient.
|
Tell the examiner you would like to do the relevant examination.
|
Examination Relevant to Cerebellar System
Check cranial nerves (cerebellopontine angle tumors).
|
Auscultate over cerebellum (for A-V malformations).
|
Fundoscopy (papilloedema).
|
Auscultate for carotid bruit (vertebra-basilar insufficiency).
|
Auscultate lung fields (bronchogenic carcinoma leading to pareneoplastic syndrome).
|
Look for the pes cavas (Friedrich’s ataxia).
|
Look for signs of hypothyroidism.
|
Other neurological examination.
|
How to Describe Brief Neurological Examination?
Here follows the description of brief neurological examination of a normal person.
“A young, conscious, co-operative gentle man lying/sitting comfortably in the bed. He is well-oriented in time, place and person. He has no obvious speech abnormality.
On examination of the cranial nerves, patient has no visible ptosis or squint; patient has normal visual acuity and normal field of vision in both eyes. Pupils are equally reactive to light and accommodation bilaterally and are normal in size. Fundi are normal. Patient has no extra-ocular opthalmoplegia or nystagmus. Corneal and conjunctival reflexes are preserved and patient has normal facial sensations. Power of the masseter muscle is normal bilaterally. Patient does not have deviation of mouth to either side and nasolabial folds are preserved. Patient can wrinkle his forehead and power of orbicularis oculi is normal. On examining the mouth, soft palate moves normally and uvula is central in position. Gag reflex is intact and on protrusion of tongue there are no fasciculations or deviation of tongue. Power of trapezius is normal.
Patient has soft neck (or no neck stiffness).
On examining the upper limbs, there is no postural abnormality, no obvious wasting or fasciculations. Muscle bulk is symmetrically normal bilaterally in all muscle groups. Tone is normal in all muscle groups at all joints bilaterally. Power is 5/5 in all muscle groups at all joints bilaterally. Deep tendon reflexes (biceps, triceps and supinator) are preserved (Grade 2) on both sides. There is no finger-nose ataxia. Sensations of fine touch, pain, vibration and temperature are intact in both upper limbs.
On examining the lower limbs, there is no obvious posture abnormality, gross wasting or fasciculations. There is no muscle tenderness and muscle bulk is symmetrically normal on both sides. Tone is normal in all muscle groups at all joints bilaterally. Tone is normal at all joints and power is 5/5 in all muscle groups (both proximal and distal) at all joints on both sides. Knee jerk and ankle jerk are well preserved i.e. grade 2 and no patellar or ankle clonus was elicited. Plantars are down going on both sides and patient has no heel-shin ataxia. Patient can easily stand from sitting position and has no obvious gait-abnormality. Sensations of fine-touch, vibration, pain, temperature and joint position are intact on both sides.”
Exercise no.1
Prepare your own check list for the command: Perform Neurological Examination of an Unconscious Patient.
Prepare your check list for the command: Examine the Sensory System of Lower Limbs.
Prepare a check list for the command: Examine the Dorsal Column Tract of this Patient.
Perform the neurological examination of a patient with some neurological deficit and write down your findings.
Examination of the Precordium
Introduction and consent
|
Greet the patient.
|
Introduce yourself and develop the rapport.
|
Get the Consent.
|
Position the patient at 45°.
|
Expose the part to be examined. If female, ask for screen and a female attendant.
|
Inspection
|
Stand at the right side of the patient and inspect.
|
Move to foot end and again have a look.
|
Inspect the neck (JVP, pulsations) and epigastrium.
|
Palpation
|
Ask for tenderness before you palpate, note if any.
|
Palpate for the apex beat (now called PMI or Point of Maximum Impulse) on left side of the chest.
|
Palpate for the left parasternal heave.
|
Palpate for epigastric pulsations.
|
Palpate base of the heart (Pulmonary & Aortic area).
|
Palpate the carotids (one at a time).
|
Palpate the trachea (especially if PMI is displaced).
|
Auscultation
|
Always time heart cycle by placing your thumb on carotids.
|
Auscultate Mitral area:
|
|
|
Auscultate while patient holds his breath during Expiration.
|
|
Auscultate with bell with patient supine and then on left lateral position.
|
|
Auscultate axilla with diaphragm of your stethoscope if systolic murmer is heard.
|
Auscultate Tricuspid area with diaphragm and ask patient to hold the breath during Inspiration.
|
Auscultate Pulmonary area during normal breathing and during Inspiration.
|
Auscultate Aortic area:
|
|
|
A2 in leaning forward position
|
Auscultate carotids
|
Conclude
|
Redrap the patient and say thanks.
|
Tell examiner that you would like to perform some relevant examination (depending upon findings).
|
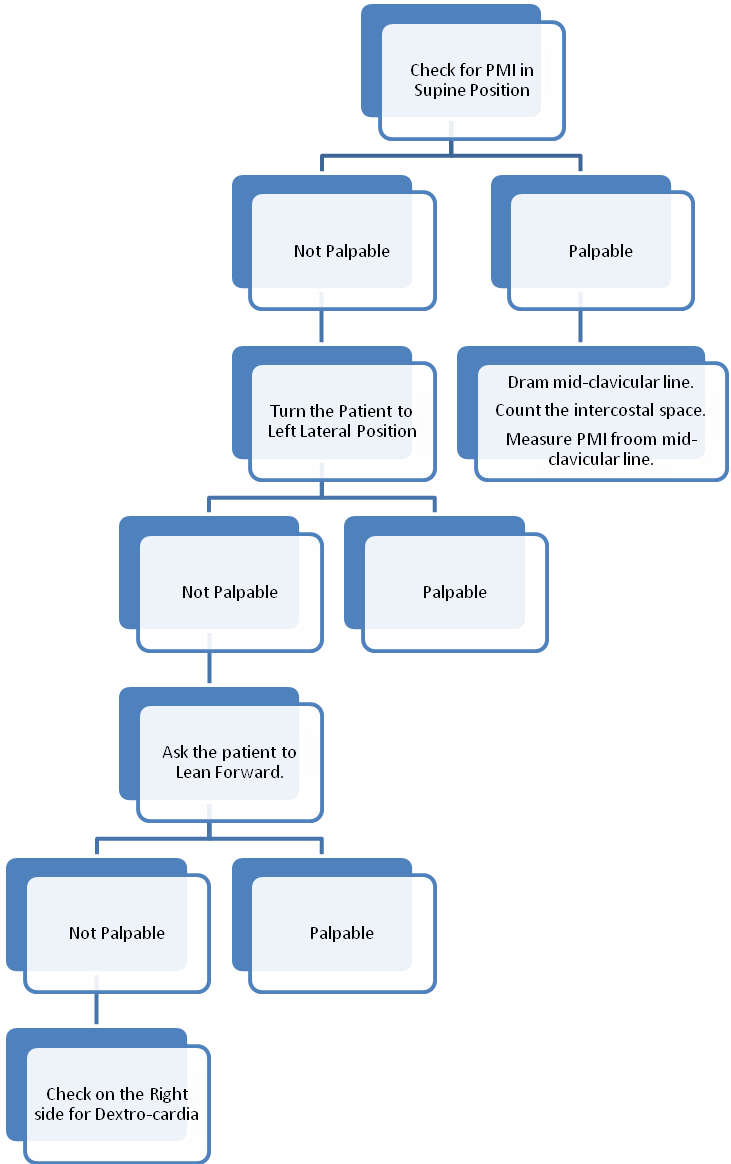
Figure 1: Localizing the PMI (Point of Maximum Impulse) or Apex Beat.
How to Describe Precordial Examination?
Description of Examination of a Normal Person
“A young conscious and co-operative gentle man is lying comfortably in bed. Patient has no obvious chest deformity, no scar mark or visible pulsations. JVP is not raised (tell in centimeters if you have measured it). There are no visible pulsations in the neck.
Patient has no chest tenderness and apex beat (PMI) is palpable in left 5th intercostals space 1cm medial to mid-clavicular line. It is neither tapping nor heaving in character. There is no palpable left parasternal heave and no palpable thrill in tricuspid, pulmonary and aortic area. Trachea is central in position.
On auscultation, rhythm appears to be regular and S1 & S2 are of normal intensity. There appears to be normal splitting of the 2nd heart sound during inspiration.
I could not appreciate any murmur or pericardial rub or 3rd or 4th heart sounds (or gallop rhythm).
There is no carotid bruit.”
Description of a Patient with Mitral Stenosis
“A young conscious co-operative female is lying uncomfortably in the bed. She has no obvious chest deformity, scar mark, prominent veins or visible pulsations. JVP is raised about 8cm of Water from sterna angle at 45° position.
Patient has no chest tenderness. Apex beat (PMI) is localized in left 5th intercostals space 2cm medial to mid-clavicular line and it is tapping in character.
There is a palpable left parasternal heave and palpable second heart sound at pulmonary area, but there is no thrill in tricuspid or aortic areas. There are no palpable epigastric pulsations.
On auscultation, rhythm appears to be normal. Patient has loud S1 and loud pulmonary component of 2nd heart sound but no gallop rhythm. There is an opening snap followed by a mid-diastolic low-pitched crescendo-decresendo rumbling murmur best heard at mitral area in left lateral position, more prominent during expiration with pre-systolic accentuation. No murmur is heard at tricuspid, pulmonary or aortic area. There is no carotid bruit and patient does not have hoarse voice.
Sir, I would like to perform relevant examination.”
Exercise
Prepare a check list for the command: Examine the Base of the Heart.
Prepare check list for the command: Examine the Pulse of the Patient.
Prepare check list for the command: Perform the General Physical Examination relevant to Cardiovascular System.
Perform the examination of Pre-cordium of a patient with Valvular Heart Disease along with the Relevant Examination and write down the Description.
Respiratory System
Prepare check list for the command: Examine the Front of the Chest.
Prepare check list for the command: Examine the Back of the Chest.
Description: Examination of Front of the Chest in a Normal Person.
“A young conscious cooperative gentle man lying comfortably in the bed. He appears not to be in distress and his respiratory rate is 14/min and it is abdomino-thoracic. Patient has no visible chest deformity, pulsations or scar mark. JVP is not raised. Patient does not have pursed lips or cyanosis.
On palpation, trachea is slightly towards right side and apex beat is in left 5th intercostals space 1cm medial to mid-clavicular line. (There is no palpable left partasternal heave). Chest expansion is symmetrically normal on both sides and it was measured to be 4.5cm. Patient has normal vocal fremitus.
Percussion note is normally resonant on both sides of the chest anteriorly and upper border of the liver is in right 4th intercostals space.
Patient has normal vesicular breathing on both sides and there are no added (adventitious) sounds. Vocal resonance is normal on both lung fields and whispering pectoriloque is not present.”
0 COMMENTS:
Post a Comment